Addressing challenges together – whether with one’s partner, family members, co-workers, or, in unprecedented times, with a whole nation – begins with self-kindness.
The Self-Kindness Group for Virginia residents meets on Thursdays from 5:30 to 6:45 PM EDT.
- Fees are pay-what-you-can up to the standard fee of $45 per group session.
- I offer self-pay counseling services and do not accept health insurance.
- Virginia residency and registration are required. Attendees must register as clients and sign consent forms to participate in online counseling.
- Please contact me to register for the group or with any questions you may have.
Self-kindness provides an inner sense of safety and strength from which one can powerfully contribute to teamwork. The self-judgment and self-reprimand inherent in “tough love” – widely believed to be motivating – actually can cause immobilizing despair.
Self-kindness begins with a self-hug.

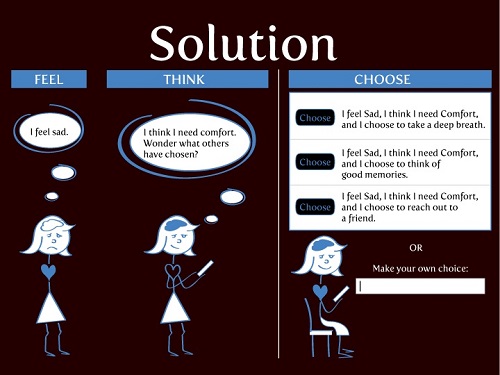
The top-recommended counseling protocol for anxiety, depression, and many mental health challenges is cognitive behavior therapy (CBT). Using CBT, one becomes aware of one’s feelings and thoughts and challenges unhelpful beliefs with facts. The next step is self-support.
The Self-Kindness Group will focus on the self-support skills offered by CBT. Here’s the group’s mission: Learn and practice skills to address troubling feelings, thoughts, words, and actions that arise in troubling times. Here’s more information about this and other groups and here’s the meeting protocol we use.
I wish I could open this group to everyone. However, national licensing for counselors is not available in the United States. I am licensed to practice counseling in the Commonwealth of Virginia only.
Avoiding troubling realities is human and humane. When avoidance becomes the go-to, it becomes both a cause and symptom of many mental health challenges. We may all need extra support as staying in our homes may require us to approach what we’ve avoided for awhile.
We’ll also need a sense of humor.
If you would like to find an image on the Internet that you like, please compose an awareness-themed caption for it. (For ideas, check out the Awareness Skills and Awareness Skills Curriculum pages under the Resources menu on our site.)
Serious is good, but funny is better. Here are my examples. I invite you to best them!
Example #1: Image
Caption: “You’re a dog named Issues?! I’ve been avoiding you!”
Example #2: Image
Caption: “Volume control?! I don’t need no stinkin’ volume control!”
Please have your image’s URL and your caption ready to copy and paste into the chat at 5:30 PM!
To register for the Self-Kindness Group, other groups, or to request other counseling services, please learn more about appointments and fees, then use our contact form to send me your email address. I will email registration information through our client portal.
If you have questions, please feel free to contact me. Anyone, anywhere is welcome to use any of the materials that might be helpful to them under the Resources menu.
If you reside in Virginia and this is a fit for you, I welcome seeing you and sharing kindness with you online!
Image: iStock
This post originally announced the inaugural session of the Self-Kindness Group. Here is the introduction to self-kindness that we discussed in the first group. This post was last updated on 4/10/20.
The views expressed are mine alone and do not necessarily reflect the positions of my colleagues, clients, family members, or friends. This content is for informational purposes only and is not a substitute for medical or professional advice. Consult a qualified health care professional for personalized medical and professional advice.





{kind=link}